
Epidemiology and Risk Factors
Embryology and Pathophysiology
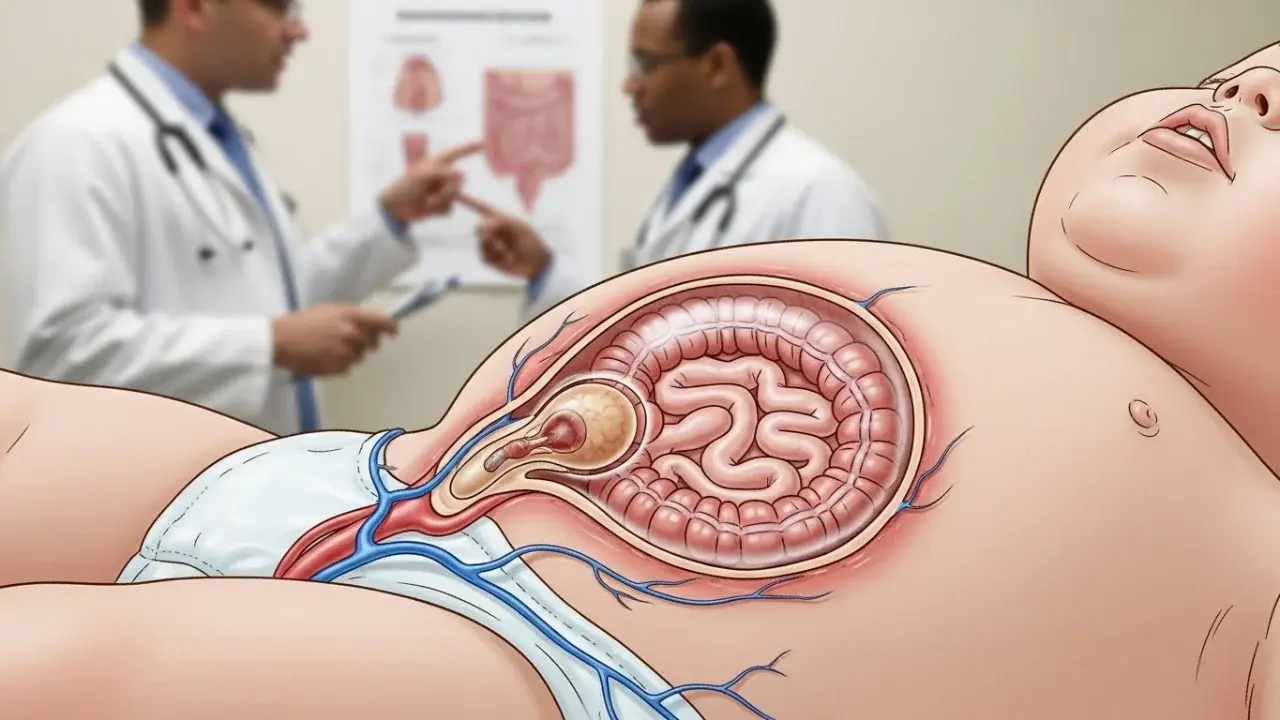
Understanding gastroshiza requires an appreciation of embryonic development. During early gestation, the intestines of the developing fetus temporarily herniate into the umbilical cord before returning to the abdominal cavity. Gastroschisis occurs when the abdominal wall fails to close completely, typically to the right of the umbilical cord, allowing the intestines—and occasionally the stomach, liver, or other organs—to remain outside the abdominal cavity. The precise cause of this defect is not fully understood, though theories suggest that vascular disruptions or abnormal development of the body wall may play a role.
Because the intestines are directly exposed to amniotic fluid, which contains enzymes and other substances, prolonged exposure can lead to inflammation, thickening, and even damage of the bowel. This can impact intestinal function after birth, sometimes necessitating long-term medical management.
Diagnosis and Prenatal Detection
To comprehend gastroshiza, one has to acknowledge embryonic development first. The intestines of the fetus in the early stages of pregnancy go out to the umbilical cord but later return to the belly. When the abdominal wall does not close completely, which is usually the case to the right side of the umbilical cord, then this condition called gastroschisis occurs, and baby’s intestines, and sometimes other organs such as the stomach, liver, etc., remain outside the abdomen. No one is exactly sure which factors lead to this malformation, but there are some theories about it like vascular disruption or body wall abnormal development. Given that the intestines are directly exposed to the amniotic fluid, which is enriched with enzymes and other substances, if the exposure lasts for a longer period, the intestines may get inflamed, thickened, or even damaged. This may have a negative impact on the functioning of the intestines after the baby is born which may sometimes require the baby to be under medical care for a long time.

Delivery Considerations
Detection of gastroshiza before birth has become much easier with the aid of modern imaging methods. A high-resolution ultrasound, which is usually done during the second trimester, can show that the intestines are outside the fetal abdomen. The most important indications of the diagnosis are the loops of the bowel that are floating in the amniotic fluid and the umbilical cord that is intact. Gastroshiza is generally to the right of the umbilical cord and does not have a membrane covering it, whereas omphalocele does. The early recognition of the condition is very important to draw up a delivery and a post-natal care plan. Sometimes fetal MRI is done to get more precise pictures of the abdominal contents and decide the extent of bowel involvement. Prenatal diagnosis also opens up the opportunity for the involved teams of obstetricians, neonatologists, and pediatric surgeons to plan the multidisciplinary care thereby enhancing the results.
Surgical Management
Surgery is the cornerstone of gastroshiza management. The objective is to return the protruding organs to the abdominal cavity and close the defect while avoiding complications such as bowel compression or compromised blood flow. Surgical strategies depend on the size of the defect and the condition of the intestines:
-
Primary Closure: If the abdominal cavity can accommodate the intestines without excessive pressure, a single surgery is performed shortly after birth to return the organs and close the abdominal wall. This approach is preferred but may not always be possible.
-
Staged Repair (Silo Technique): In cases where the intestines are swollen or the defect is large, surgeons may use a sterile pouch called a silo to gradually return the intestines over several days. This method reduces tension on the abdominal wall and allows the organs to adapt to the confined space.
Postoperative care is critical and typically involves total parenteral nutrition (TPN) while the bowel recovers its normal function. Feeding is gradually introduced once bowel motility returns. In some cases, prolonged intestinal dysmotility or short bowel syndrome may occur, requiring extended medical management.
Complications and Prognosis
While modern surgical techniques have significantly improved survival rates, gastroshiza can be associated with complications:
-
Infections: Due to exposed intestines and surgical interventions.
-
Intestinal Atresia or Stenosis: Portions of the bowel may be narrowed or absent, complicating digestion.
-
Feeding Difficulties: Some infants experience delayed bowel function, necessitating prolonged TPN.
-
Growth and Developmental Delays: Rare but possible, especially in cases with prolonged hospital stays.
Fortunately, with early detection, skilled surgical care, and comprehensive neonatal support, the survival rate for infants with gastroshiza exceeds 90% in high-resource settings. Long-term outcomes are generally favorable, although some children may require ongoing nutritional support or follow-up surgeries.
Prevention and Future Directions
There is still no sure way to stop gastroshiza, as the cause is not yet known. Nevertheless, among the public health measures, it is a good idea to recommend people to give up smoking and refrain from drinking alcohol during the first stages of pregnancy since these might lower the risk. Along with the research which is being done on the causes of defects of the abdominal wall in terms of environmental and molecular factors, there is a hope of preventing them in future through new methods. Byfocusing on different specialisation combined with the improvement of surgical techniques and neonatal care, the outcomes of the newborns affected by the problem are getting better gradually day by day. Furthermore, cutting-edge prenatal imaging and monitoring technologies have enabled better planning of delivery and immediate postnatal intervention, thus assisting in the reduction of infant morbidity and mortality.
Conclusion
Gastroshiza is a very rare but also a very serious birth defect that imposes extraordinary challenges in terms of diagnosis, birthing, and the care of the baby after birth. For example, the process of prenatal imaging, expert surgical management, and all-round neonatal support are the ones to thank for leading to positive outcomes. While the exact cause of this condition is still a mystery, the advances in medicine have turned the gastroshiza issue from a life-threatening condition into one that has a high likelihood of survival and a good long-term prognosis. The affected families can benefit from early intervention and multidisciplinary care, thus being provided with a window to see just how far the neoteric and sophisticated neonatal and pediatric surgery has come.